A practical guide for parents and caregivers managing type 1 diabetes in children, covering blood sugar targets, insulin types, school management, DKA warning signs, and emotional support.
Type 1 diabetes in children is an autoimmune condition in which the pancreas stops producing insulin. Without it, blood sugar rises to dangerous levels. Managing T1D in a child involves daily blood sugar monitoring, multiple daily insulin doses or an insulin pump, carbohydrate awareness, and close coordination with a diabetes care team. With the right tools and support, children with T1D live full, active lives.
- At a Glance: Type 1 diabetes in children is an autoimmune condition, not caused by diet or lifestyle, and requires lifelong insulin therapy.
- The ADA recommends blood sugar targets of 70 to 180 mg/dL (3.9 to 10.0 mmol/L) before and after meals for most children, though targets vary by age and situation.
- Blood sugar checks are needed multiple times daily; many families use continuous glucose monitors (CGMs) to reduce fingerstick frequency.
- DKA (diabetic ketoacidosis) is a life-threatening emergency in children with T1D; early warning signs include vomiting, deep rapid breathing, and fruity breath.
- School management requires a written Diabetes Medical Management Plan (DMMP) shared with teachers and the school nurse.
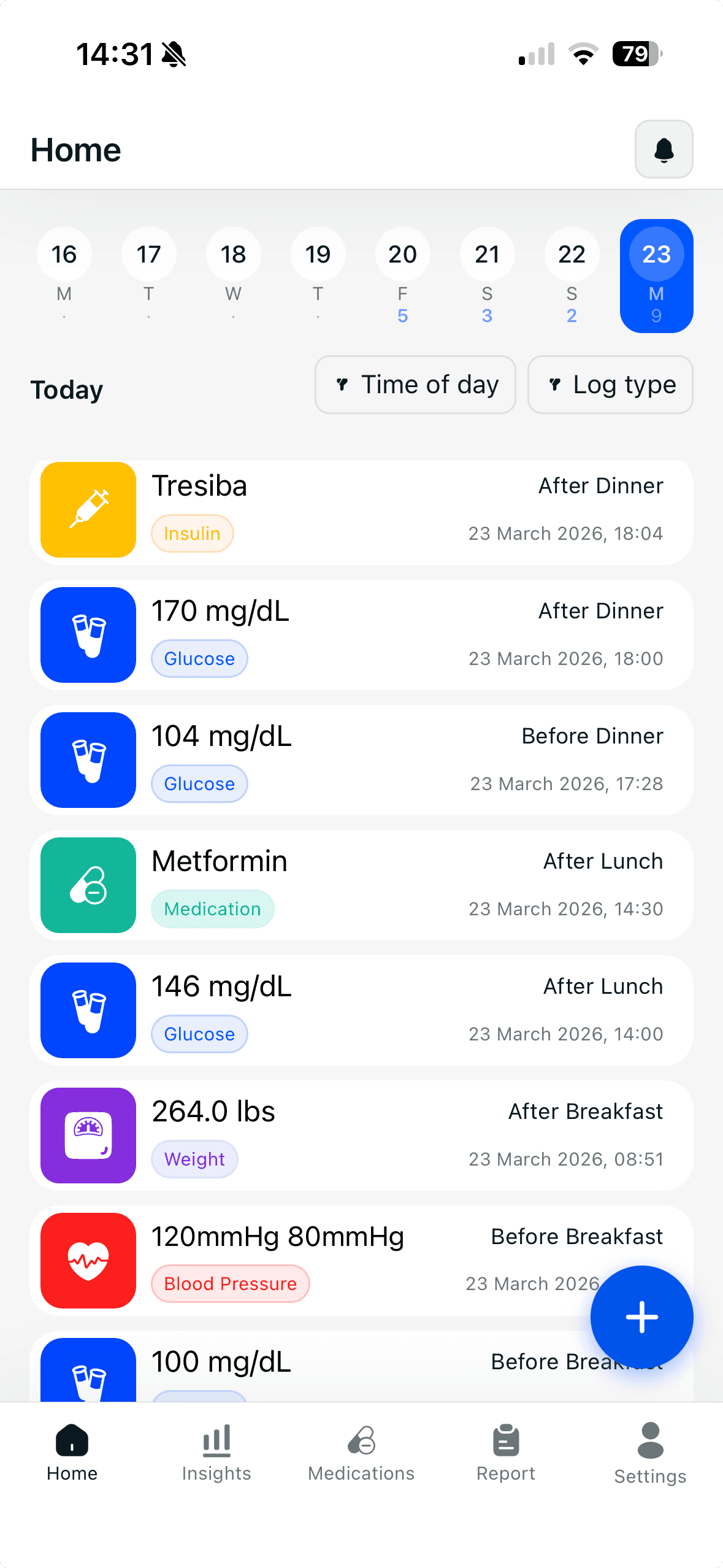
- Glucoly allows parents and caregivers to log readings, track insulin, and export PDF reports for medical appointments.
Type 1 vs. Type 2 Diabetes in Children: Key Differences
Type 1 and type 2 diabetes are distinct conditions with different causes, management approaches, and trajectories. Understanding the difference is essential for caregivers.
- Type 1 diabetes is autoimmune: the immune system destroys the insulin-producing beta cells in the pancreas. The cause is genetic and environmental, not lifestyle or diet. Insulin therapy is required from diagnosis and cannot be replaced by diet or exercise alone.
- Type 2 diabetes in children involves insulin resistance and is strongly associated with obesity, physical inactivity, and family history. It can sometimes be managed with lifestyle changes and oral medications, at least initially.
- T1D in children typically presents suddenly with rapid weight loss, extreme thirst, frequent urination, and vomiting. Symptoms often develop over days to weeks. Type 2 in children is usually detected through screening, with few or no symptoms.
- T1D accounts for the majority of diabetes diagnoses in children under 10. Type 2 in children is most common in adolescents.
- Both types require blood sugar monitoring, but insulin therapy and the intensity of management are typically far greater in T1D.
Blood Sugar Targets for Children with T1D by Age (ADA Guidelines)
The American Diabetes Association provides blood sugar targets for children with type 1 diabetes. These targets balance tight glucose control with the risk of hypoglycemia, which is a particular concern in young children who cannot reliably communicate symptoms.
- General ADA target for most children: before meals 80 to 130 mg/dL (4.4 to 7.2 mmol/L); bedtime and overnight 80 to 140 mg/dL (4.4 to 7.8 mmol/L). These are individualized targets; your care team may set different values.
- A1C target for most children with T1D: below 7.0%, per ADA 2024 Standards of Care. Some guidelines suggest below 7.5% for younger children where hypoglycemia risk is a greater concern.
- Time in Range (TIR): the ADA recommends a TIR of over 70% for glucose readings between 70 and 180 mg/dL (3.9 to 10.0 mmol/L) as a complementary goal when using a CGM.
- Younger children and toddlers require more conservative targets to prevent severe hypoglycemia, as they are less able to communicate early symptoms.
- Targets should be individualized by your child's diabetes care team based on age, hypoglycemia history, and access to CGM technology.
Insulin Types Used in Children with Type 1 Diabetes
Children with T1D require both basal insulin to cover background glucose needs and bolus insulin to cover meals and corrections. The specific types used depend on the child's regimen and whether they use an insulin pump.
- Rapid-acting insulin (bolus): used before meals and for blood sugar corrections. Examples include insulin aspart (NovoLog/NovoRapid), insulin lispro (Humalog), and insulin glulisine (Apidra). Onset is typically 10 to 15 minutes, with peak action at 1 to 2 hours.
- Long-acting or basal insulin: provides a steady background level throughout the day and night. Examples include insulin glargine (Lantus, Basaglar, Toujeo), insulin detemir (Levemir), and insulin degludec (Tresiba).
- Insulin pumps (CSII): deliver rapid-acting insulin continuously through a small catheter, replacing both basal and bolus injections. Many modern pumps work with CGMs to automatically adjust delivery (hybrid closed-loop systems).
- Ultra-rapid insulins (Fiasp, Lyumjev): newer formulations that act faster than standard rapid-acting insulin, often used in pumps or for children with unpredictable eating patterns.
- All insulin dosing in children must be prescribed and managed by a pediatric endocrinologist or certified diabetes care team. Never adjust doses without medical guidance.
School Management Tips for Children with T1D
School presents unique management challenges: children spend long hours away from their caregivers, engage in unpredictable physical activity, and face social pressures around eating and injections. Preparation and communication make a significant difference.
- Create a written Diabetes Medical Management Plan (DMMP): this document, signed by your child's doctor, specifies blood sugar targets, testing frequency, insulin doses, hypoglycemia treatment steps, and emergency contacts. Provide copies to the school nurse and classroom teacher.
- Under Section 504 of the Rehabilitation Act in the United States, children with diabetes are entitled to reasonable accommodations, including permission to check blood sugar and eat in class, bathroom access, and time for low blood sugar treatment.
- Designate trained staff members who can assist with blood sugar checks and administer glucagon in an emergency, not only the school nurse.
- Ensure the school has adequate supplies: fast-acting glucose (juice boxes, glucose tablets), a glucagon kit, spare meter strips, and insulin pen or pump supplies.
- Discuss exercise management proactively: PE classes, sports, and field trips all require adjustments. Send a pre-adjusted snack and brief low treatment plan with your child for any active day.
- Communicate regularly with school staff, especially as the child grows and insulin needs change.
Recognizing DKA (Diabetic Ketoacidosis) Early
Diabetic ketoacidosis (DKA) is a life-threatening complication that occurs when insulin levels are severely insufficient, causing the body to break down fat at a dangerous rate and produce acidic ketones. DKA is more common in children with T1D than in adults and can develop rapidly.
- Early warning signs: blood sugar above 250 mg/dL (13.9 mmol/L), moderate or large ketones on a urine or blood ketone test, nausea, and vomiting.
- Progressing signs: abdominal pain, deep and rapid breathing (Kussmaul breathing), a sweet or fruity smell on the breath, and extreme fatigue.
- Late or severe DKA signs: confusion, difficulty staying awake, and loss of consciousness. This is a medical emergency requiring immediate hospital care.
- Test for ketones whenever your child's blood sugar exceeds 250 mg/dL (13.9 mmol/L), especially during illness or if an insulin pump fails.
- Never give extra rapid-acting insulin and wait at home if ketones are moderate or large and the child is vomiting. Go to the emergency room.
- DKA prevention: never skip insulin doses, check for pump site failures daily, and establish a sick day management plan with your care team in advance.
Emotional and Psychological Aspects of T1D in Children
Living with T1D places a significant emotional burden on children and caregivers alike. Research published in Diabetes Care consistently shows elevated rates of anxiety, depression, and diabetes distress in youth with T1D and their parents. Addressing the psychological dimension of the condition is as important as glucose control.
- Diabetes distress: worry about glucose management, fear of hypoglycemia, and the relentlessness of daily tasks are normal and valid responses. Distress is distinct from clinical depression but warrants attention.
- Fear of hypoglycemia: particularly common in parents of young children. This fear can lead to keeping blood sugar deliberately higher than recommended, which increases long-term complications risk. CGM use and family education can help.
- Children often feel different or singled out around food, injections, and glucose checks. Role-play, peer support groups, and open conversation help children normalize the condition.
- Seek a referral to a mental health professional with diabetes experience if your child shows persistent sadness, social withdrawal, refusing to check blood sugar, or signs of disordered eating around insulin.
- Caregiver burnout is real. Parents of children with T1D report significantly higher rates of sleep disruption, anxiety, and burnout than parents of children without diabetes. Building a support network, including diabetes parent groups, is important for long-term sustainability.
How Glucoly Helps Families Track and Share Data
Managing T1D in a child means coordinating data across multiple caregivers, school staff, and a medical team. Glucoly is designed to make that coordination straightforward.
- Log all readings in one place: manual glucose entries, insulin doses (basal and bolus), and weight are stored in a single timeline, making it easy to review what happened and when.
- CGM integration: Glucoly syncs with Dexcom and Libre data through Apple Health, automatically pulling readings without manual entry.
- Before and after meal tagging: identify post-meal spikes and understand how specific meals affect your child's blood sugar over time.
- Doctor-ready PDF export: generate a complete glucose, insulin, and trend report for your child's pediatric endocrinologist appointment. This saves clinic time and gives your care team the data they need to make dose adjustments.
- Trend windows of 7, 14, 30, and 90 days show whether time-in-range and overall control are improving or need attention.
- Smart reminders: set reminders for scheduled blood sugar checks, insulin doses, and medication times so nothing gets missed during a busy school or activity day.
This article is for general education and is not a substitute for medical advice. Consult your healthcare provider before making changes to your child's treatment plan. Type 1 diabetes management in children requires ongoing supervision by a qualified pediatric endocrinologist or diabetes care team.
Frequently Asked Questions
What age does type 1 diabetes typically appear in children?
- T1D can appear at any age, but peak onset in children occurs between ages 4 to 7 and again during puberty (10 to 14 years), according to the ADA.
- Puberty-related hormonal changes increase insulin resistance, making blood sugar management more challenging for adolescents with T1D.
- The condition is increasingly diagnosed in adults as well. Adult-onset T1D (including LADA, latent autoimmune diabetes in adults) is often initially misdiagnosed as type 2.
- Early symptoms in children include rapid-onset extreme thirst, frequent urination, unexpected weight loss, and vomiting. If you observe these signs, seek medical care immediately.
Can a child outgrow type 1 diabetes?
- No. Type 1 diabetes is a lifelong condition. The autoimmune destruction of insulin-producing beta cells is permanent.
- Some children experience a 'honeymoon phase' shortly after diagnosis, during which the remaining beta cells produce limited insulin and reduce insulin requirements temporarily. This phase typically lasts weeks to months.
- Research into beta cell replacement therapies, including islet cell transplantation and artificial pancreas systems, continues to advance. However, no cure is available as of 2026.
- With optimal management, children with T1D grow normally, participate in all activities, and face good long-term outcomes.
Is a CGM necessary for a child with T1D?
- CGMs are not legally required, but the ADA strongly recommends them for all people with T1D who can access and afford one, including children.
- Multiple studies show CGM use significantly improves time in range and A1C while reducing severe hypoglycemia and DKA rates in children.
- CGMs also reduce the number of daily fingerstick checks needed, which is particularly beneficial for young children who find multiple daily tests distressing.
- Popular CGMs for children include the Dexcom G6 and G7 (which do not require calibration fingersticks) and the Abbott Freestyle Libre 3.
- Glucoly syncs with Dexcom and Libre data via Apple Health, making it a useful companion to CGM use for families who want trend analysis and medical reporting alongside real-time CGM alerts.
Track your blood sugar and spot patterns with Glucoly - free on iOS and Android.
Download Glucoly